Patient 3: An Elderly Woman with Sjögren’s Syndrome With Pill Swallowing Difficulty
Patient Background
This is the case of an 81-year-old woman with a history of Sjögren’s syndrome, leading to severe dry mouth, difficulty swallowing pills, and chronic bloating with early satiety. She was frail, weighing only 85 pounds, and struggled to gain weight despite efforts to increase her caloric intake.
Her medical history included:
- Autoimmune disease (Sjögren’s syndrome)
- Osteoporosis
- Chronic foot pain from neuropathy of unclear cause
- Severe sedentary lifestyle due to foot pain
Prior extensive workup included:
- CT Abdomen/Pelvis: moderate to large colonic stool burden; excessive gastric gas attributed to aerophagia (air swallowing)
- Upper Endoscopy: mild chronic gastritis; negative for H. pylori
- Gastric Emptying Study: Normal
Despite multiple specialist evaluations, no definitive cause was found for her symptoms, and many attributed her issues to the underlying Sjögren’s syndrome.
Dietary history included:
- Breakfast: almond milk with collagen and toast (butter, peanut butter, or maple syrup).
- Meals: overnight oats, rice, chicken, fish, meat, vegetables, berries, apples, bananas.
- Frequent snacking (cake, ice cream) in efforts to gain weight.
She had previously tried prescription-strength digestive enzymes without benefit, and it actually worsened her symptoms. A prior SIBO breath test at another medical center had been reported as negative.
On physical examination, her abdomen was moderately distended and had mild diffuse tenderness to palpation.
Treatment: Implementing Dr. Rajsree’s 4-Phase SIBO Protocol
Phase 1-2: Promote Motility and Reduce Gas Level:
At her initial visit, she had already independently begun parts of Dr. Rajsree’s 4-Phase SIBO Protocol, including:
- Essential Magnesium 2 capsules (bedtime)
- Motility Activator 1 capsule (bedtime)
- Digestive Enzyme Pro (1 capsule after meals)
Due to her difficulty swallowing, she opened the capsules and mixed the contents into applesauce — a necessary adaptation given her Sjögren’s syndrome and risk of aspiration.
Notably, she reported early improvements:
- Increased bowel regularity
- New ability to pass gas (which she could not do previously), a sign of improved gut motility.
Dietary Strategy:
She began a low FODMAP / low lectin SIBO diet, with specific instructions to practice meal spacing:
- Avoid snacking between meals
- Maintain 4–5 hours between meals
- Maintain a 12-hour overnight fast between dinner and breakfast
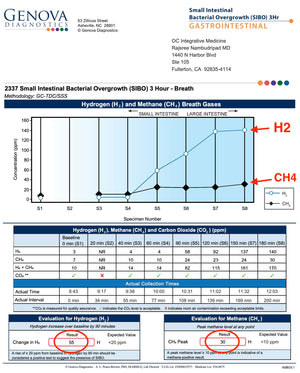
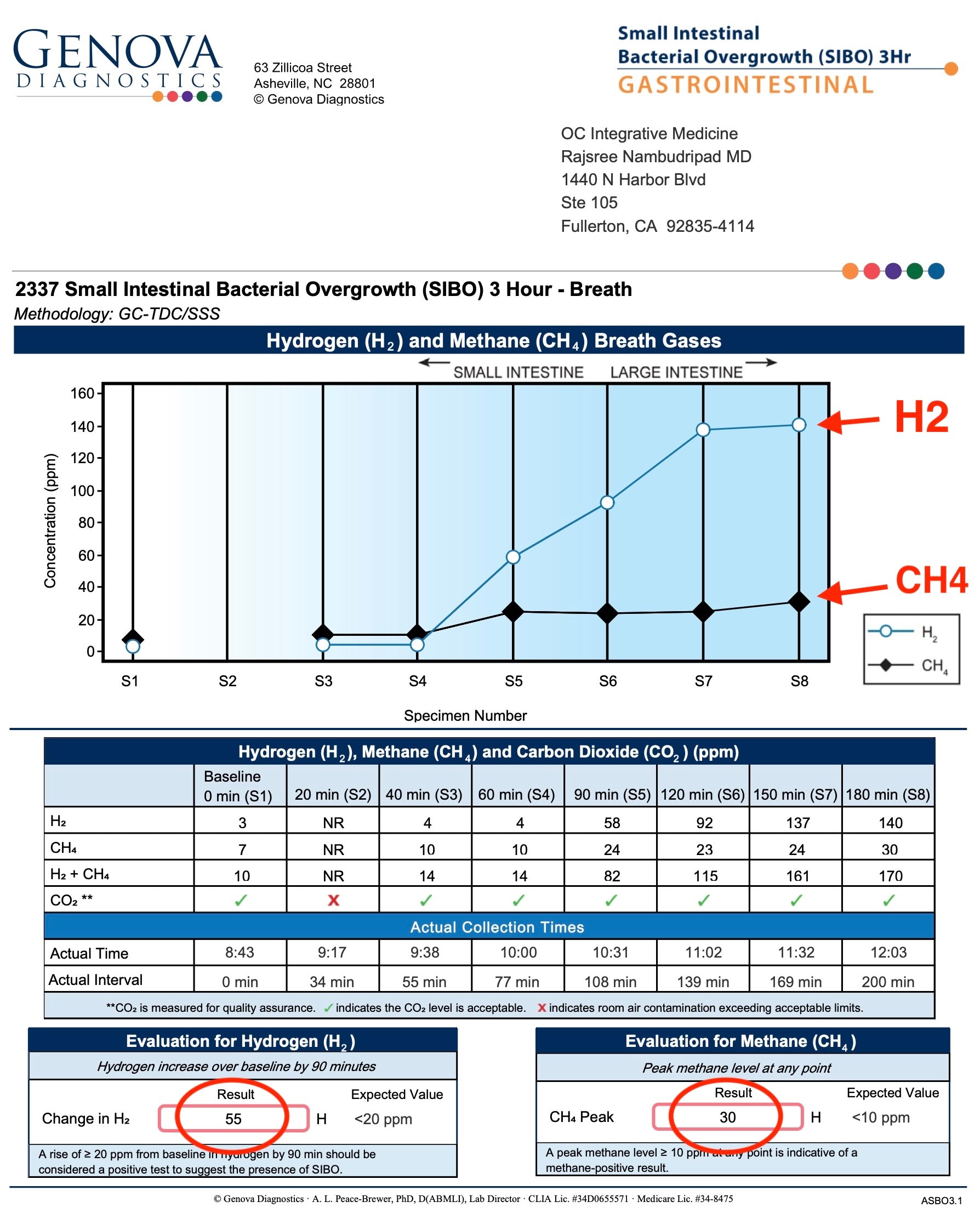
SIBO Breath Testing
At her follow up visit, a lactulose breath test revealed:
- Hydrogen (H₂): 55 ppm
- Methane (CH₄): 30 ppm (Intestinal Methanogen Overgrowth)
This was diagnostic for mixed-type SIBO (both hydrogen and methane elevation). The Intestinal Methanogen Overgrowth (IMO) was likely contributing to her constipation.

Phase 4: Targeted Herbal Antimicrobials
Despite swallowing difficulties, we carefully initiated the antimicrobial phase by:
Addition of:
- Berberine Pro, Oregano Oil, and Allicidin. She opened the capsules and mixed the contents into applesauce (twice daily after food)
To simplify her regimen and reduce pill burden:
- We omitted Spore Probiotic IgG from her protocol
- Elemental diet supplementation using Physician’s Elemental Diet (Dextrose Free) by Integrative Therapeutics (a powder that can be mixed with water) was used to supplement her calories for additional nutrition support.
Implementation was very gradual to accommodate her sensitive constitution.
Outcomes
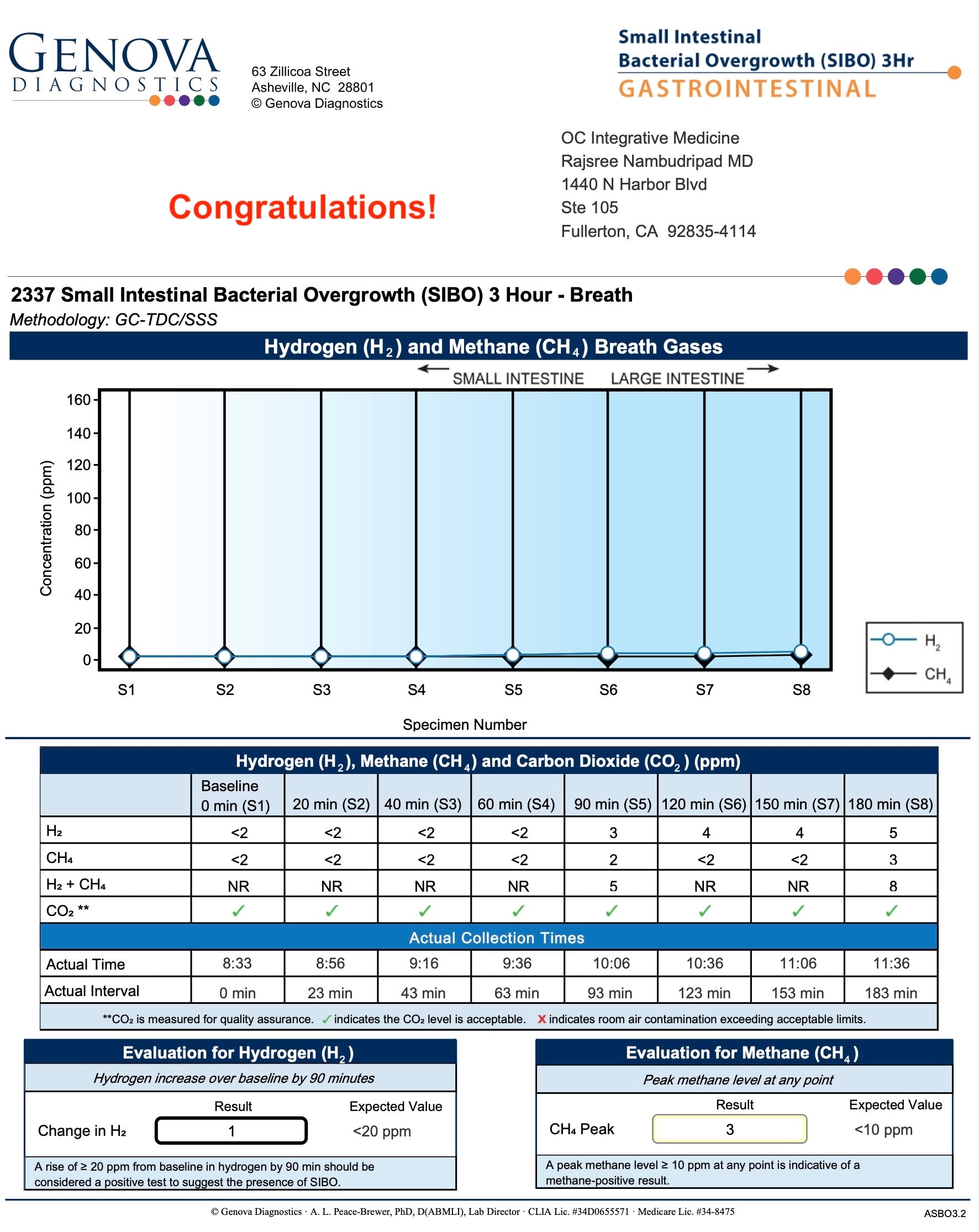
After six weeks herbal antimicrobials, her repeat SIBO breath test showed:
- Hydrogen (H₂): decreased from 55 ppm → 1 ppm
- Methane (CH₄): decreased from 30 ppm → 3 ppm

Clinically, she achieved:
- Improved bowel regularity with 2 capsules of Essential Magnesium
- Significant reduction in bloating
- Improved appetite, allowing her to eat larger meals
- A modest but meaningful weight gain of a few pounds
Maintenance Plan
Following successful eradication of SIBO, she transitioned to the Prevention of Relapse phase of Dr. Rajsree’s 4-Phase SIBO Protocol:
- Initiated Probiotic 100 Billion (for broad-spectrum microbiome support)
- Continued Digestive Enzyme Pro with meals
- Continued Essential Magnesium and Motility Activator at bedtime
- She began reintroducing small amounts of fermented foods (including goat kefir) to promote gut resilience
Special emphasis remained on gradual dietary expansion and maintaining meal spacing.
Key Insights
This case demonstrates that even frail, elderly patients with significant swallowing difficulties can achieve complete SIBO resolution when a Dr. Rajsree’s SIBO protocol is carefully implemented under a doctor’s supervision.
Adaptations, such as opening capsules into applesauce, gradual titration of antimicrobials, and strategic dietary support, were key to her success.
Root causes of her SIBO likely included:
- Impaired intestinal motility related to Sjögren’s syndrome
- Possible pancreatic enzyme insufficiency (common in Sjögren’s)
- Sedentary lifestyle affecting gut movement
Interestingly, Digestive Enzyme Pro was well-tolerated and highly effective for her — whereas previous prescription-strength digestive enzymes had worsened her symptoms.
The supportive involvement of her family was also critical to her adherence and overall success.
Patient Background
This is the case of an 81-year-old woman with a history of Sjögren’s syndrome, leading to severe dry mouth, difficulty swallowing pills, and chronic bloating with early satiety. She was frail, weighing only 85 pounds, and struggled to gain weight despite efforts to increase her caloric intake.
Her medical history included:
- Autoimmune disease (Sjögren’s syndrome)
- Osteoporosis
- Chronic foot pain from neuropathy of unclear cause
- Severe sedentary lifestyle due to foot pain
Prior extensive workup included:
- CT Abdomen/Pelvis: moderate to large colonic stool burden; excessive gastric gas attributed to aerophagia (air swallowing)
- Upper Endoscopy: mild chronic gastritis; negative for H. pylori
- Gastric Emptying Study: Normal
Despite multiple specialist evaluations, no definitive cause was found for her symptoms, and many attributed her issues to the underlying Sjögren’s syndrome.
Dietary history included:
- Breakfast: almond milk with collagen and toast (butter, peanut butter, or maple syrup).
- Meals: overnight oats, rice, chicken, fish, meat, vegetables, berries, apples, bananas.
- Frequent snacking (cake, ice cream) in efforts to gain weight.
She had previously tried prescription-strength digestive enzymes without benefit, and it actually worsened her symptoms. A prior SIBO breath test at another medical center had been reported as negative.
On physical examination, her abdomen was moderately distended and had mild diffuse tenderness to palpation.
Treatment: Implementing Dr. Rajsree’s 4-Phase SIBO Protocol
Phase 1-2: Promote Motility and Reduce Gas Level:
At her initial visit, she had already independently begun parts of Dr. Rajsree’s 4-Phase SIBO Protocol, including:
- Essential Magnesium 2 capsules (bedtime)
- Motility Activator 1 capsule (bedtime)
- Digestive Enzyme Pro (1 capsule after meals)
Due to her difficulty swallowing, she opened the capsules and mixed the contents into applesauce — a necessary adaptation given her Sjögren’s syndrome and risk of aspiration.
Notably, she reported early improvements:
- Increased bowel regularity
- New ability to pass gas (which she could not do previously), a sign of improved gut motility.
Dietary Strategy:
She began a low FODMAP / low lectin SIBO diet, with specific instructions to practice meal spacing:
- Avoid snacking between meals
- Maintain 4–5 hours between meals
- Maintain a 12-hour overnight fast between dinner and breakfast
SIBO Breath Testing
At her follow up visit, a lactulose breath test revealed:
- Hydrogen (H₂): 55 ppm
- Methane (CH₄): 30 ppm (Intestinal Methanogen Overgrowth)
This was diagnostic for mixed-type SIBO (both hydrogen and methane elevation). The Intestinal Methanogen Overgrowth (IMO) was likely contributing to her constipation.
Phase 4: Targeted Herbal Antimicrobials
Despite swallowing difficulties, we carefully initiated the antimicrobial phase by:
Addition of:
- Berberine Pro, Oregano Oil, and Allicidin. She opened the capsules and mixed the contents into applesauce (twice daily after food)
To simplify her regimen and reduce pill burden:
- We omitted Spore Probiotic IgG from her protocol
- Elemental diet supplementation using Physician’s Elemental Diet (Dextrose Free) by Integrative Therapeutics (a powder that can be mixed with water) was used to supplement her calories for additional nutrition support.
Implementation was very gradual to accommodate her sensitive constitution.
Outcomes
After six weeks herbal antimicrobials, her repeat SIBO breath test showed:
- Hydrogen (H₂): decreased from 55 ppm → 1 ppm
- Methane (CH₄): decreased from 30 ppm → 3 ppm
Clinically, she achieved:
- Improved bowel regularity with 2 capsules of Essential Magnesium
- Significant reduction in bloating
- Improved appetite, allowing her to eat larger meals
- A modest but meaningful weight gain of a few pounds
Maintenance Plan
Following successful eradication of SIBO, she transitioned to the Prevention of Relapse phase of Dr. Rajsree’s 4-Phase SIBO Protocol:
- Initiated Probiotic 100 Billion (for broad-spectrum microbiome support)
- Continued Digestive Enzyme Pro with meals
- Continued Essential Magnesium and Motility Activator at bedtime
- She began reintroducing small amounts of fermented foods (including goat kefir) to promote gut resilience
Special emphasis remained on gradual dietary expansion and maintaining meal spacing.
Key Insights
This case demonstrates that even frail, elderly patients with significant swallowing difficulties can achieve complete SIBO resolution when a Dr. Rajsree’s SIBO protocol is carefully implemented under a doctor’s supervision.
Adaptations, such as opening capsules into applesauce, gradual titration of antimicrobials, and strategic dietary support, were key to her success.
Root causes of her SIBO likely included:
- Impaired intestinal motility related to Sjögren’s syndrome
- Possible pancreatic enzyme insufficiency (common in Sjögren’s)
- Sedentary lifestyle affecting gut movement
Interestingly, Digestive Enzyme Pro was well-tolerated and highly effective for her — whereas previous prescription-strength digestive enzymes had worsened her symptoms.
The supportive involvement of her family was also critical to her adherence and overall success.