Patient 11: Mixed IBS (IBS-M) and Mixed-Type SIBO
Patient Background
This is the case of a 43-year-old woman who presented with a long-standing history of irritable bowel syndrome dating back to 2005. Her symptoms initially began as IBS-D, later shifted toward IBS-C, and ultimately evolved into IBS-M with alternating diarrhea and constipation.
Over time, her symptoms became increasingly severe and disruptive to daily life. She reported a notable worsening following a major lifestyle and career change—from a highly active profession as a dancer and choreographer to a significantly more sedentary and stressful role as a second-grade teacher. In parallel, she noticed that her IBS flares became strongly associated with her menstrual cycle, with predictable exacerbations around her periods.
She described episodes of severe abdominal pain that were so intense that even sound or vibration worsened her symptoms, forcing her to lie completely still. These attacks lasted anywhere from 15 minutes to 2 hours. Between episodes, she continued to experience daily bloating and abdominal distension, often describing herself as “looking pregnant” when bloated.
Symptom Profile
Her symptoms included:
- Severe abdominal bloating and visible distension
- Alternating diarrhea and constipation (IBS-M)
- Episodic severe abdominal pain attacks
- Hormonal symptom flares around menstruation
- Food-triggered symptoms, particularly with:
- Dairy
- Oatmeal
- Suspected gluten sensitivity
- Sensation of phlegm in the throat, later suspected to be related to low stomach acid
During menstrual flares, she noted that eating cucumbers helped calm her gastrointestinal symptoms.
Past Medical History
- IBS-M
- Thyroid nodule (monitored by endocrinology)
- IgE testing positive only to kidney bean (Class 1)
Prior Dietary Interventions
She had previously followed a low-FODMAP diet in an effort to control symptoms. While this reduced some bloating, it led to an unintended 9–10 lb weight loss and did not fully resolve her IBS. Due to ongoing symptoms, she felt increasingly restricted in her diet and anxious about food choices.
On physical examination, her abdomen was moderately distended and had mild diffuse tenderness to palpation.
Patient was underweight weighing 100 lbs at 5'3", with a BMI of 17.
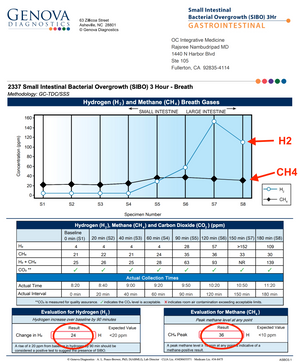
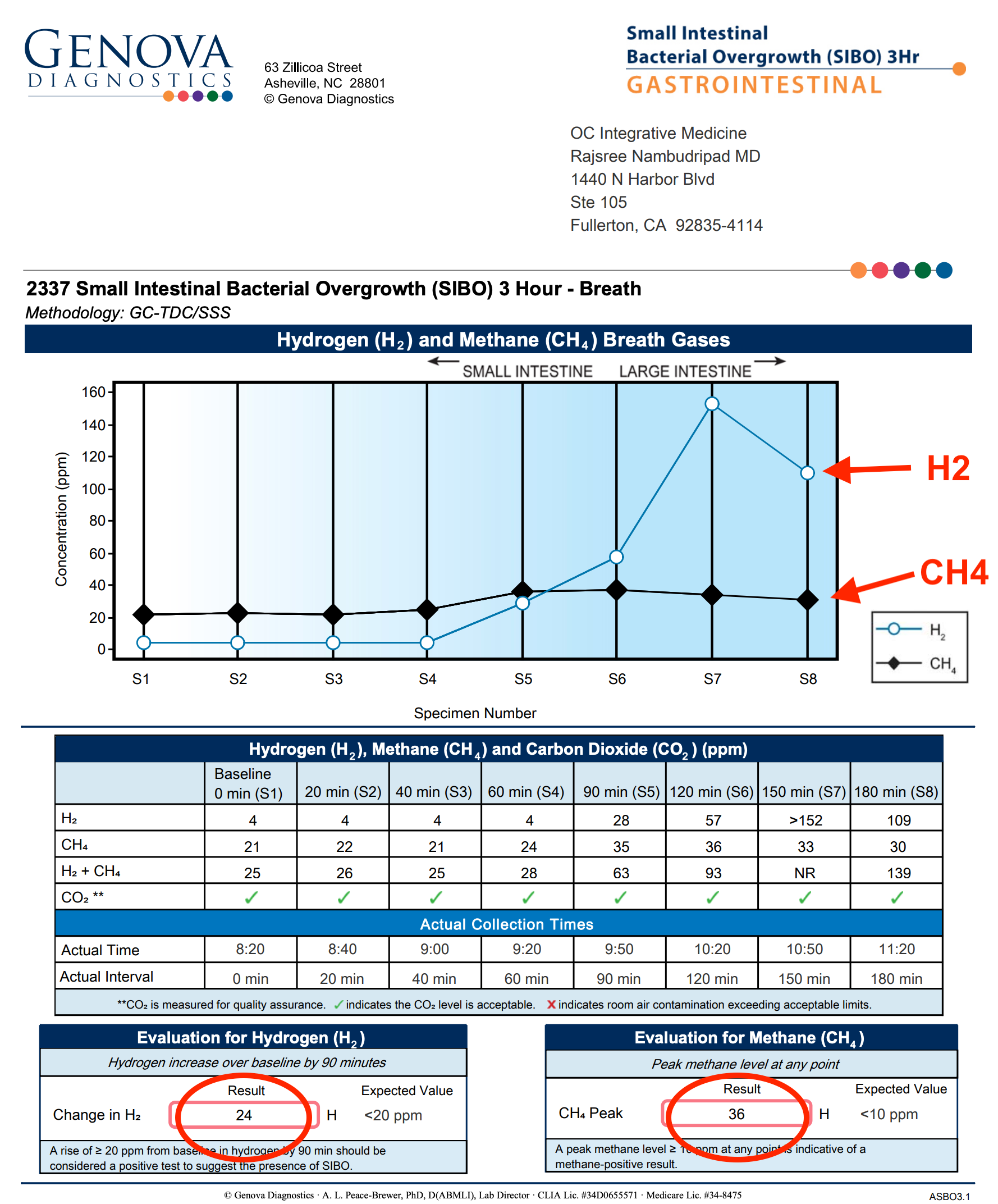
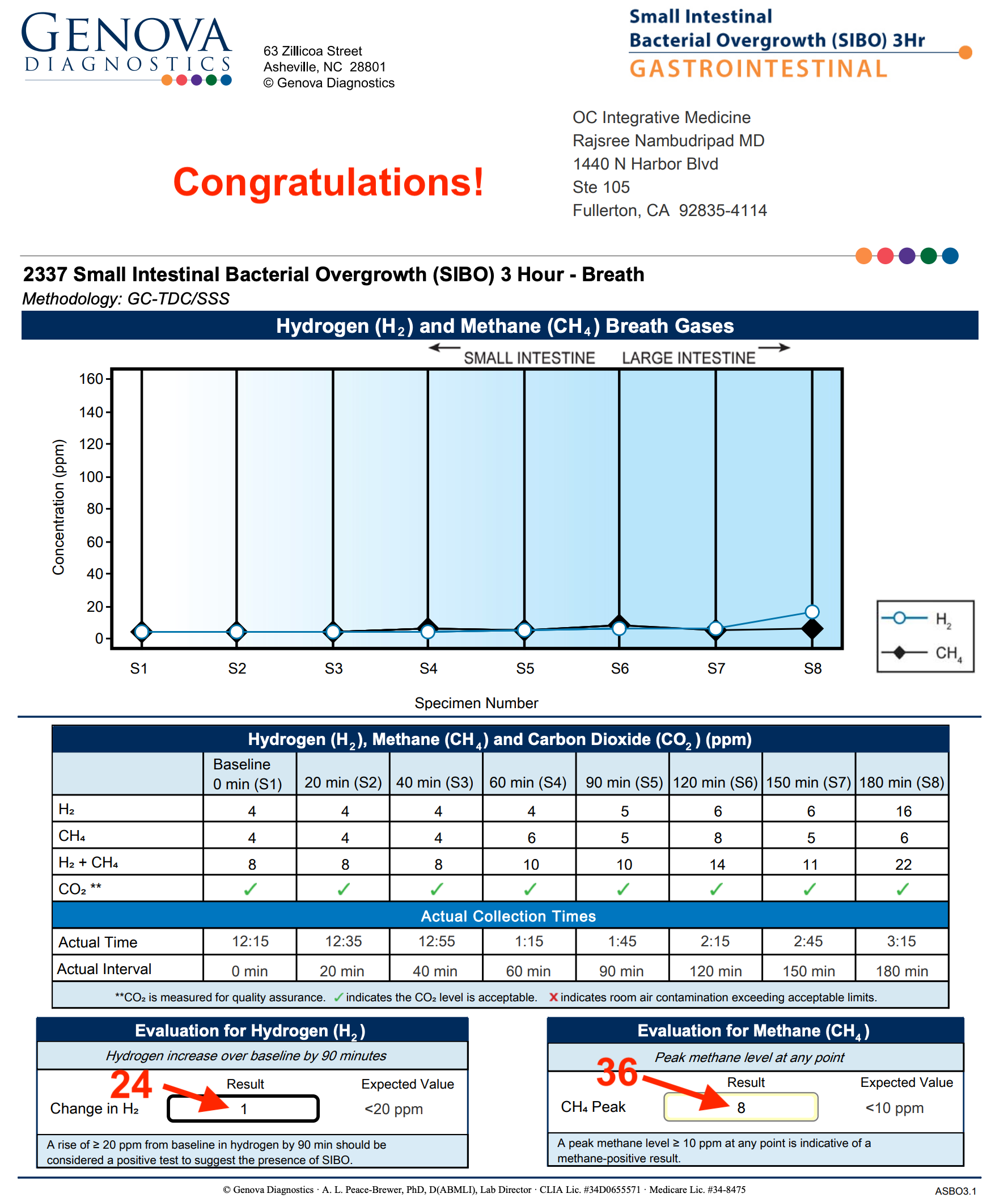
SIBO Breath Testing
Lactulose breath testing revealed:
- Hydrogen (H₂): 24 ppm
- Methane (CH₄): 36 ppm
These findings were diagnostic for mixed-type SIBO, consistent with her alternating bowel habits and mixed IBS presentation.

Treatment: Implementing Dr. Rajsree’s Herbal Protocol for SIBO
She was placed on Dr. Rajsree’s Herbal SIBO Protocol, with emphasis on restoring motility, and improving digestion.
Phase 1-2: Promote Motility and Reduce Gas Levels
- Digestive Enzyme Pro (2 capsules after meals)
- Betaine & Pepsin (1-2 capsules after meals)
- Essential Magnesium (up to 4 capsules at bedtime)
- Motility Activator (1 capsule at bedtime)
Dietary Strategy:
She began a low FODMAP / low lectin SIBO diet, with specific instructions to practice meal spacing:
- Avoid snacking between meals
- Maintain 4–5 hours between meals
- Maintain a 12-hour overnight fast between dinner and breakfast
Nutritional Support During Treatment
Due to progressive weight loss and risk of becoming underweight, the Elemental Diet was incorporated strategically during treatment to support nutrition and prevent further weight loss. This provided calories while minimizing digestive burden and fermentation during antimicrobial therapy.
Phase 3-4: Reduce Inflammation and Herbal Antimicrobial Therapy
Addition of:
- Spore Probiotic IgG in AM on empty stomach
- Herbal antimicrobials:
- Berberine Pro, Oregano Oil, and Allicidin (1 capsule each after every meal) for 6 weeks
Follow-Up and Outcomes
After 6 weeks of herbal antimicrobials:
- Hydrogen (H₂): decreased from 24 ppm → 1 ppm
- Methane (CH₄): decreased from 36 ppm → 8 ppm

Clinically, she experienced:
- Resolution of IBS symptoms
- Significant reduction in bloating and abdominal distension
- Normalization of bowel habits (1–2 bowel movements daily)
- Improved tolerance of meals
Although she lost approximately 10 pounds during treatment, the use of elemental nutrition helped stabilize her intake, and she was able to regain weight after completing therapy.
Food Reintroduction Strategy
After completing 4–6 weeks of treatment, she began a structured food reintroduction plan:
- Foods were added back one at a time
- Each food was trialed for 2-3 days before introducing the next
- This approach allowed identification of triggers while minimizing relapse risk
She remained somewhat sensitive to certain foods but continued to expand her diet gradually.
Additional Insight: Low Stomach Acid
Persistent throat phlegm raised concern for hypochlorhydria. The addition of Betaine with Pepsin led to significant improvement, supporting low stomach acid as a contributing factor to her digestive dysfunction and SIBO risk.
Maintenance Plan
Following successful eradication of SIBO, she transitioned into the Prevention of Relapse phase of Dr. Rajsree’s protocol:
- Continued Digestive Enzyme Pro and Betaine & Pepsin with meals
- Continued Essential Magnesium and Motility Activator at bedtime
- Transitioned from Spore Probiotic IgG to Probiotic 100 Billion for broad-spectrum microbiome support
- Ongoing gradual dietary expansion
Key Insights
This case illustrates how mixed-type IBS (IBS-M) often reflects mixed-type SIBO, underscoring the importance of breath testing rather than symptom-based assumptions.
Contributing root causes likely included:
- Impaired intestinal motility related to chronic stress and reduced physical activity
- Possible low stomach acid contributing to bacterial overgrowth and food intolerance
Despite significant symptom severity and weight loss, this patient responded extremely well to Dr. Rajsree’s 4-Phase SIBO Herbal Protocol. Treatment led to normalization of her SIBO breath test, resolution of IBS symptoms, improved food tolerance, and restoration of weight—without the use of pharmaceutical antibiotics.
This case further highlights the importance of sequencing treatment properly: supporting motility and digestion first, using targeted herbal antimicrobials, protecting nutrition during therapy, and implementing a slow, structured food reintroduction to prevent relapse.
Patient Background
This is the case of a 43-year-old woman who presented with a long-standing history of irritable bowel syndrome dating back to 2005. Her symptoms initially began as IBS-D, later shifted toward IBS-C, and ultimately evolved into IBS-M with alternating diarrhea and constipation.
Over time, her symptoms became increasingly severe and disruptive to daily life. She reported a notable worsening following a major lifestyle and career change—from a highly active profession as a dancer and choreographer to a significantly more sedentary and stressful role as a second-grade teacher. In parallel, she noticed that her IBS flares became strongly associated with her menstrual cycle, with predictable exacerbations around her periods.
She described episodes of severe abdominal pain that were so intense that even sound or vibration worsened her symptoms, forcing her to lie completely still. These attacks lasted anywhere from 15 minutes to 2 hours. Between episodes, she continued to experience daily bloating and abdominal distension, often describing herself as “looking pregnant” when bloated.
Symptom Profile
Her symptoms included:
- Severe abdominal bloating and visible distension
- Alternating diarrhea and constipation (IBS-M)
- Episodic severe abdominal pain attacks
- Hormonal symptom flares around menstruation
- Food-triggered symptoms, particularly with:
- Dairy
- Oatmeal
- Suspected gluten sensitivity
- Sensation of phlegm in the throat, later suspected to be related to low stomach acid
During menstrual flares, she noted that eating cucumbers helped calm her gastrointestinal symptoms.
Past Medical History
- IBS-M
- Thyroid nodule (monitored by endocrinology)
- IgE testing positive only to kidney bean (Class 1)
Prior Dietary Interventions
She had previously followed a low-FODMAP diet in an effort to control symptoms. While this reduced some bloating, it led to an unintended 9–10 lb weight loss and did not fully resolve her IBS. Due to ongoing symptoms, she felt increasingly restricted in her diet and anxious about food choices.
On physical examination, her abdomen was moderately distended and had mild diffuse tenderness to palpation.
Patient was underweight weighing 100 lbs at 5'3", with a BMI of 17.
SIBO Breath Testing
Lactulose breath testing revealed:
- Hydrogen (H₂): 24 ppm
- Methane (CH₄): 36 ppm
These findings were diagnostic for mixed-type SIBO, consistent with her alternating bowel habits and mixed IBS presentation.
Treatment: Implementing Dr. Rajsree’s Herbal Protocol for SIBO
She was placed on Dr. Rajsree’s Herbal SIBO Protocol, with emphasis on restoring motility, and improving digestion.
Phase 1-2: Promote Motility and Reduce Gas Levels
- Digestive Enzyme Pro (2 capsules after meals)
- Betaine & Pepsin (1-2 capsules after meals)
- Essential Magnesium (up to 4 capsules at bedtime)
- Motility Activator (1 capsule at bedtime)
Dietary Strategy:
She began a low FODMAP / low lectin SIBO diet, with specific instructions to practice meal spacing:
- Avoid snacking between meals
- Maintain 4–5 hours between meals
- Maintain a 12-hour overnight fast between dinner and breakfast
Nutritional Support During Treatment
Due to progressive weight loss and risk of becoming underweight, the Elemental Diet was incorporated strategically during treatment to support nutrition and prevent further weight loss. This provided calories while minimizing digestive burden and fermentation during antimicrobial therapy.
Phase 3-4: Reduce Inflammation and Herbal Antimicrobial Therapy
Addition of:
- Spore Probiotic IgG in AM on empty stomach
- Herbal antimicrobials:
- Berberine Pro, Oregano Oil, and Allicidin (1 capsule each after every meal) for 6 weeks
Follow-Up and Outcomes
After 6 weeks of herbal antimicrobials:
- Hydrogen (H₂): decreased from 24 ppm → 1 ppm
- Methane (CH₄): decreased from 36 ppm → 8 ppm
Clinically, she experienced:
- Resolution of IBS symptoms
- Significant reduction in bloating and abdominal distension
- Normalization of bowel habits (1–2 bowel movements daily)
- Improved tolerance of meals
Although she lost approximately 10 pounds during treatment, the use of elemental nutrition helped stabilize her intake, and she was able to regain weight after completing therapy.
Food Reintroduction Strategy
After completing 4–6 weeks of treatment, she began a structured food reintroduction plan:
- Foods were added back one at a time
- Each food was trialed for 2-3 days before introducing the next
- This approach allowed identification of triggers while minimizing relapse risk
She remained somewhat sensitive to certain foods but continued to expand her diet gradually.
Additional Insight: Low Stomach Acid
Persistent throat phlegm raised concern for hypochlorhydria. The addition of Betaine with Pepsin led to significant improvement, supporting low stomach acid as a contributing factor to her digestive dysfunction and SIBO risk.
Maintenance Plan
Following successful eradication of SIBO, she transitioned into the Prevention of Relapse phase of Dr. Rajsree’s protocol:
- Continued Digestive Enzyme Pro and Betaine & Pepsin with meals
- Continued Essential Magnesium and Motility Activator at bedtime
- Transitioned from Spore Probiotic IgG to Probiotic 100 Billion for broad-spectrum microbiome support
- Ongoing gradual dietary expansion
Key Insights
This case illustrates how mixed-type IBS (IBS-M) often reflects mixed-type SIBO, underscoring the importance of breath testing rather than symptom-based assumptions.
Contributing root causes likely included:
- Impaired intestinal motility related to chronic stress and reduced physical activity
- Possible low stomach acid contributing to bacterial overgrowth and food intolerance
Despite significant symptom severity and weight loss, this patient responded extremely well to Dr. Rajsree’s 4-Phase SIBO Herbal Protocol. Treatment led to normalization of her SIBO breath test, resolution of IBS symptoms, improved food tolerance, and restoration of weight—without the use of pharmaceutical antibiotics.
This case further highlights the importance of sequencing treatment properly: supporting motility and digestion first, using targeted herbal antimicrobials, protecting nutrition during therapy, and implementing a slow, structured food reintroduction to prevent relapse.